In the high-stakes environment of a pediatric emergency room, the most critical skill a junior doctor can possess is the “doorway assessment.” Before you ever touch a patient or reach for a stethoscope, you must be able to form a “first impression” of their physiological status. The Pediatric Assessment Triangle (PAT) is the internationally recognized tool designed for this exact purpose. Unlike the ABCDE approach, which requires physical contact and vital signs, the PAT is a purely observational tool. Specifically, it allows the clinician to rapidly categorize the severity of a child’s illness and determine the urgency of intervention. Consequently, mastering this visual assessment can literally mean the difference between life and death in the first thirty seconds of a clinical encounter.
The Three Pillars of the PAT
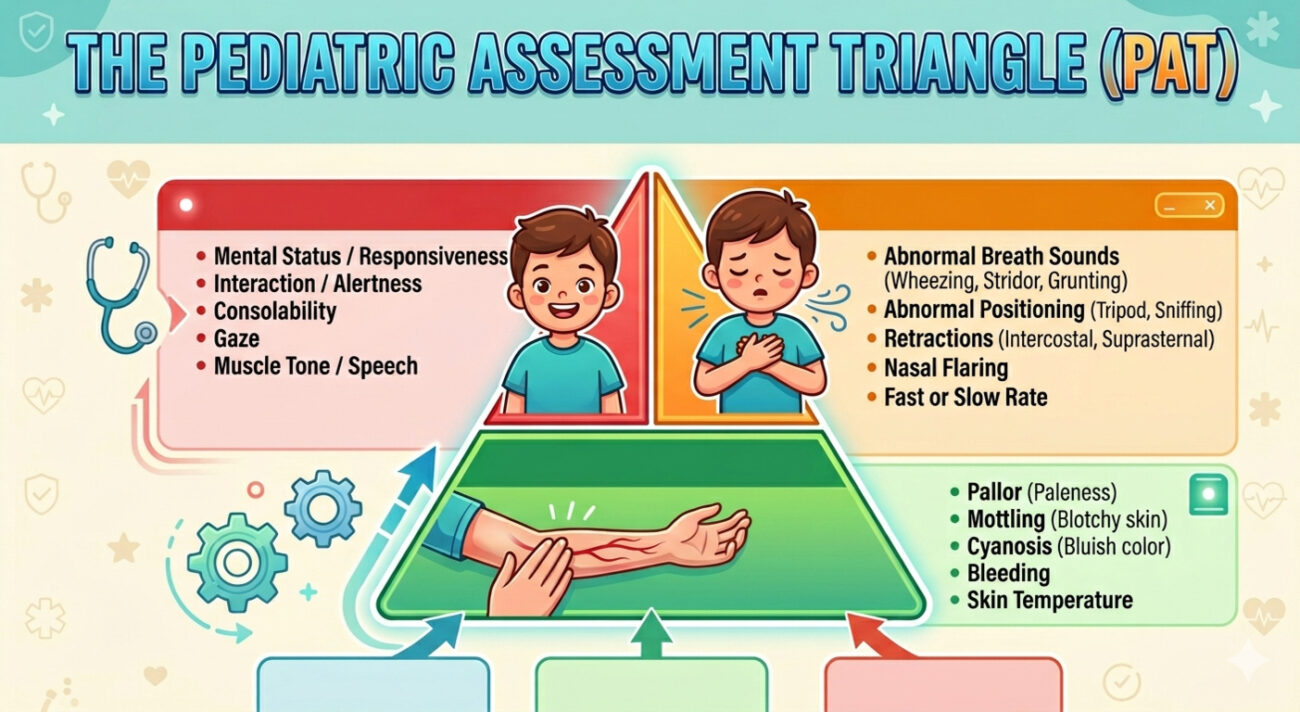
The PAT consists of three key components that, when viewed together, provide a snapshot of the child’s cardiopulmonary and neurological status. It is a “triangle” because if any one side is “broken,” the child is at risk; if multiple sides are broken, the child is in critical danger.
1. Appearance (Neurological Status)
Appearance is arguably the most important component of the triangle. It reflects the adequacy of brain perfusion, oxygenation, and central nervous system function. To remember what to look for, residents often use the TICLS mnemonic:
- T – Tone: Is the child moving spontaneously, or are they limp?
- I – Interactiveness: Are they alert and engaged with their environment?
- C – Consolability: Can the parent soothe the child, or is the crying inconsolable?
- L – Look/Gaze: Is the child making eye contact, or do they have a “glassy” stare?
- S – Speech/Cry: Is the cry strong and spontaneous, or weak and muffled?
2. Work of Breathing (Respiratory Status)
This pillar provides a visual assessment of the child’s respiratory effort. Because children have more compliant chest walls than adults, they show signs of distress much more clearly through physical effort rather than just rate. Look for:
- Abnormal Airway Sounds: Grunting, stridor, or wheezing audible without a stethoscope.
- Abnormal Positioning: “Tripoding” or “sniffing position” to open the airway.
- Retractions: Suprasternal, intercostal, or substernal pulling of the skin.
- Nasal Flaring: Widening of the nostrils during inspiration.
3. Circulation to Skin (Cardiac Status)
The skin is a non-vital organ; therefore, when the body enters shock, it diverts blood away from the skin to protect the heart and brain. By observing skin color and pattern, you can assess the adequacy of cardiac output.
- Pallor: Paleness, which may be the first sign of compensated shock.
- Mottling: A patchy, purplish discoloration indicating poor peripheral perfusion.
- Cyanosis: A blue tint to the skin or mucous membranes, indicating late-stage deoxygenation.
Interpreting the PAT: Clinical Categorization
The power of the PAT lies in its ability to generate a presumptive diagnosis based on which sides of the triangle are abnormal.
| Appearance | Work of Breathing | Circulation | Physiological Category |
| Normal | Abnormal | Normal | Respiratory Distress |
| Abnormal | Abnormal | Normal | Respiratory Failure |
| Normal | Normal | Abnormal | Compensated Shock |
| Abnormal | Normal | Abnormal | Decompensated Shock |
| Abnormal | Normal | Normal | Primary CNS/Metabolic Insult |
| Abnormal | Abnormal | Abnormal | Cardiopulmonary Failure |
Clinical Scenario: The “Limp” Infant
Consider a 10-month-old infant, Rohan, rushed into the triage area by his father. Rohan has had diarrhea for three days. As you look at him from the doorway:
- Appearance: He is limp in his father’s arms and does not look up when you call his name (Abnormal).
- Work of Breathing: His chest rise is quiet and regular with no retractions (Normal).
- Circulation: His skin looks notably pale and slightly mottled (Abnormal).
Initially, you might just think “dehydration.” However, using the PAT, you quickly identify Abnormal Appearance + Abnormal Circulation, which equals Decompensated Shock. Consequently, you bypass the triage queue, move him immediately to the resuscitation bay, and prepare for intraosseous access and fluid boluses. This rapid categorization ensures that Rohan receives life-saving treatment minutes faster than a traditional assessment would allow.
The Role of the Resident in Triage
As a resident, you must cultivate the habit of performing the PAT on every pediatric patient you see. Furthermore, you should teach this to nursing staff and interns, as it creates a standardized language for communication. Instead of saying, “The baby in bed 4 looks bad,” you can say, “The baby in bed 4 has an abnormal PAT—appearance is poor and work of breathing is increased, suggesting respiratory failure.” Therefore, the PAT serves as a bridge between visual observation and immediate clinical action.
Frequently Asked Questions
Q1: Can I use the PAT if a child is sleeping?
It is difficult to assess “Appearance” accurately in a sleeping child. If you have any concerns about the other two pillars, you should gently stimulate the child to assess their interactiveness and tone. A child who cannot be easily aroused has an “Abnormal Appearance.”
Q2: Does a normal PAT mean the child is safe to go home?
No. The PAT is a “first impression” tool to identify life-threatening illness. A child may have a normal PAT but still have an underlying condition (like an early surgical abdomen or a significant infection) that requires a full physical exam, history, and testing.
Q3: How does “Appearance” differ from “Circulation”?
Appearance is a window into the brain (CNS), while Circulation is a window into the heart (CVS). However, they are linked; poor circulation will eventually lead to poor brain perfusion and an abnormal appearance.