In clinical neurology, the physical examination is your most powerful diagnostic imaging tool. Before a patient ever enters an MRI scanner, a skilled clinician can pinpoint the exact location of a neurological deficit simply by wielding a reflex hammer and a tuning fork. For the junior doctor, mastering lesion localization is the fundamental rite of passage. The nervous system is a highly organized, topographical map; when a pathway is disrupted, it produces a highly specific constellation of physical signs. This comprehensive guide breaks down the critical distinctions between Upper Motor Neuron (UMN) and Lower Motor Neuron (LMN) lesions, while also navigating the complex clinical presentations of cerebellar and basal ganglia syndromes. By mastering these patterns, you transition from simply observing symptoms to definitively mapping the neuroaxis.
UMN vs. LMN: The Fundamental Divide
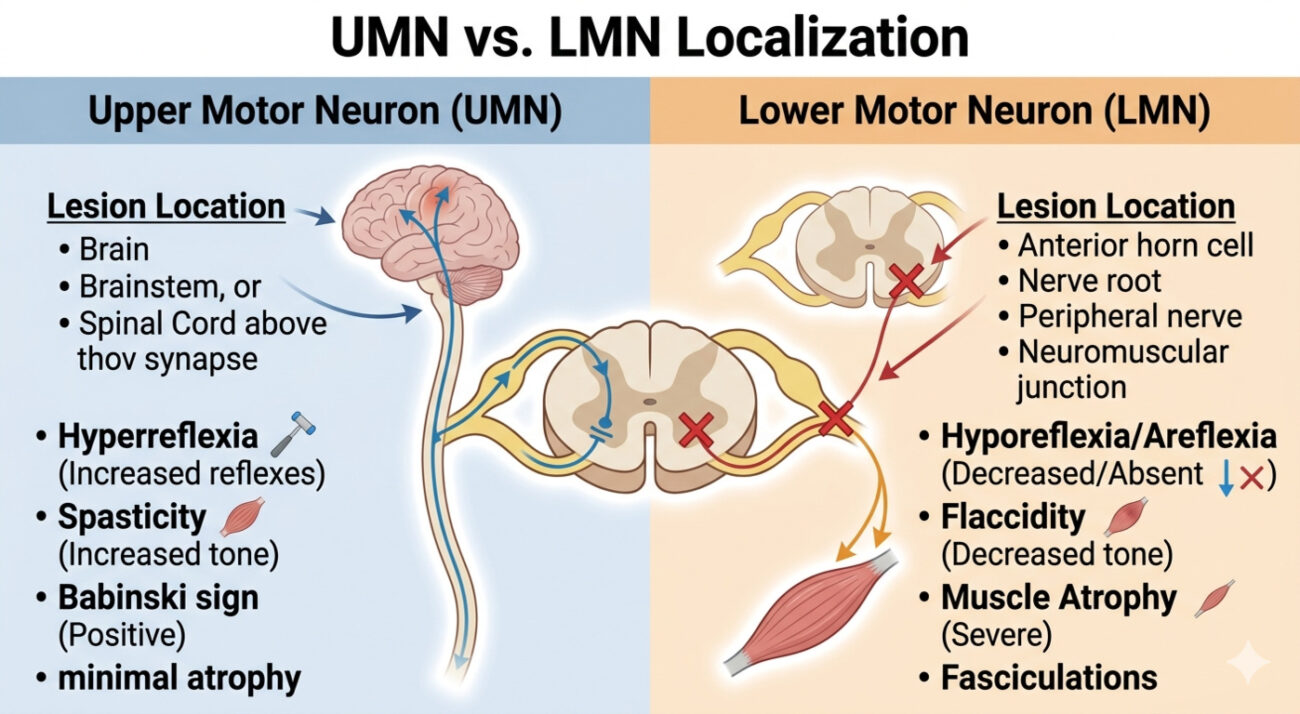
The motor system is fundamentally a two-neuron relay. The Upper Motor Neuron (UMN) originates in the cerebral cortex (specifically the precentral gyrus) and travels down the corticospinal tract, crossing over at the medulla, to synapse in the spinal cord. The Lower Motor Neuron (LMN) begins at the anterior horn cell of the spinal cord and travels out through the peripheral nerve to directly innervate the muscle.
The Clinical Signatures of Motor Lesions
The physical signs of UMN and LMN lesions are exact opposites. Recognizing these patterns allows you to instantly localize the injury to either the central nervous system (brain/spinal cord) or the peripheral nervous system (nerve root/peripheral nerve/neuromuscular junction).
| Clinical Feature | Upper Motor Neuron (UMN) Lesion | Lower Motor Neuron (LMN) Lesion |
| Muscle Tone | Increased (Spasticity / Clasp-knife) | Decreased (Flaccidity) |
| Muscle Bulk | Normal (Mild disuse atrophy late) | Pronounced and rapid atrophy |
| Reflexes | Hyperreflexia (Brisk, Clonus present) | Hyporeflexia or Areflexia |
| Fasciculations | Absent | Present (Muscle twitching) |
| Plantar Reflex | Extensor (Positive Babinski sign) | Flexor (Normal downward response) |
Cerebellar Syndromes: The Coordination Center
While the motor cortex initiates movement, the cerebellum ensures that movement is smooth, accurate, and perfectly timed. It acts as the brain’s quality control center. Crucially, cerebellar lesions produce ipsilateral (same-sided) signs because the pathways double-cross before reaching the spinal cord.
When the cerebellum is damaged (due to stroke, tumor, or toxicity), the patient does not become weak; instead, their movements become chaotic and uncoordinated. You can easily remember the classic signs of cerebellar dysfunction using the DANISH mnemonic:
- D – Dysdiadochokinesia: Inability to perform rapid, alternating movements (e.g., flipping hands back and forth).
- A – Ataxia: A wide-based, unsteady, “drunken” gait.
- N – Nystagmus: Rhythmic oscillation of the eyes, usually horizontal.
- I – Intention Tremor: A tremor that worsens dramatically as the finger approaches a target (e.g., during the finger-to-nose test).
- S – Slurred Speech: Scanning, explosive dysarthria.
- H – Hypotonia: Mild decrease in muscle tone.
Basal Ganglia Syndromes: The Movement Modulator
The basal ganglia represent the “extrapyramidal” motor system. This deep brain network acts as a volume dial for movement. It facilitates desired movements and inhibits unwanted, competing movements. Therefore, lesions here do not cause classic weakness or spasticity. Instead, they cause profound movement disorders that fall into two broad categories: hypokinetic and hyperkinetic.
Hypokinetic Syndromes (Too little movement):
Parkinson’s disease is the classic hypokinetic disorder. It occurs due to the loss of dopaminergic neurons in the substantia nigra. The hallmark signs include profound bradykinesia (slowness of movement), “cogwheel” rigidity (a ratchety resistance to passive movement), and a classic “pill-rolling” resting tremor that improves with voluntary action.
Hyperkinetic Syndromes (Too much movement):
When the inhibitory pathways of the basal ganglia are damaged, the patient experiences involuntary, extra movements. Huntington’s disease produces chorea (rapid, unpredictable, dance-like movements). Damage to the subthalamic nucleus (often due to a lacunar stroke) produces hemiballismus (violent, flinging movements of one side of the body).
Clinical Scenario: The Mixed Picture
Consider a 62-year-old man, Mr. Sharma, who presents to the clinic complaining of progressive weakness in his right hand and difficulty swallowing. During your examination, you note profound atrophy and visible fasciculations in his right thenar eminence and tongue (clear LMN signs). However, when you test his reflexes, you find a hyperactive jaw jerk, brisk knee jerks bilaterally, and a positive Babinski sign on the right (clear UMN signs).
Initially, a junior doctor might be confused by this contradictory picture. How can a patient have both flaccid, twitching muscles and spastic, hyper-reflexic responses? This unique combination of simultaneous UMN and LMN signs in the same anatomical region is the clinical hallmark of Amyotrophic Lateral Sclerosis (ALS), a devastating neurodegenerative disease that selectively attacks both motor neuron populations while sparing sensory, cerebellar, and cognitive pathways. Your precise localization directly leads to the correct, albeit grim, diagnosis.
Frequently Asked Questions
Q1: Why do UMN lesions sometimes present with initial flaccidity rather than spasticity?
Following an acute, severe UMN injury (such as a massive stroke or acute spinal cord trauma), the patient often enters a state of “spinal shock.” During this acute phase (lasting days to weeks), the affected limbs are profoundly flaccid and areflexic, mimicking an LMN lesion. Spasticity and hyperreflexia typically emerge only after the spinal circuits reorganize and become hypersensitive.
Q2: How do I easily differentiate a cerebellar tremor from a Parkinsonian tremor at the bedside?
The key is the state of the muscle during the tremor. A Parkinsonian tremor is a resting tremor; it is most prominent when the patient’s hands are resting quietly in their lap and often disappears when they reach for an object. A cerebellar tremor is an intention tremor; the limb is steady at rest, but the tremor emerges and violently worsens as the patient’s finger closes in on a target (like your finger).
Q3: What does a positive Babinski sign actually indicate anatomically?
The Babinski sign (upgoing big toe and fanning of the other toes upon stroking the lateral plantar surface of the foot) indicates structural damage specifically to the corticospinal tract. It is the most reliable, objective clinical sign of UMN dysfunction in the entire neurological examination.